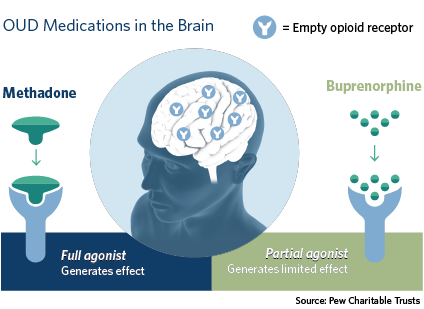
Buprenorphine is a partial opioid agonist that binds to opioid receptors in the brain, reducing cravings and withdrawal symptoms when opioids are stopped.
Buprenorphine does not have the same effects as full agonist opioids, especially when combined with naloxone.
Buprenorphine is used to treat both opioid use disorder (OUD) and chronic pain. In this continuing education program, we focus on the use of buprenorphine to treat OUD.
What is buprenorphine’s role in preventing overdose?
Buprenorphine is a key strategy to prevent overdose. As shown in the table, medications for opioid use disorder, which include buprenorphine, are listed in four of 10 of the CDC’s top recommended evidence-based strategies to prevent overdose.
CDC’s Evidence-Based Strategies for Preventing Opioid Overdose2
Carroll J, Green T, Noonan R. Evidence-Based Strategies for Preventing Opioid Overdose: What’s Working in the United States, 2018. Centers for Disease Control; 2018:40. Accessed December 2, 2019. https://www.cdc.gov/drugoverdose/pdf/pubs/2018-evidence-based-strategies.pdf
Medications for Opioid Use Disorder (MOUD)
Medications for opioid use disorder
Eliminating prior-authorization requirements for MOUD
Medications for opioid use disorder in criminal justice settings and upon release
Initiating buprenorphine-based MAT (MOUD) in emergency departments
Other Strategies
Targeted naloxone distribution
Academic detailing
Fentanyl screening
Good Samaritan Laws (immunity from prosecution for assisting a person overdosing)
Naloxone distribution in treatment centers and criminal justice settings
Syringe services programs (also known as syringe access programs)
How is it prescribed?
General guidelines
Statement
True or False
Feedback
Buprenorphine is usually prescribed as a short-term medication.
✘✔
This statement is false. Buprenorphine is typically prescribed as a long-term medication, sometimes life-long.
1
Providers are required to be registered with the DEA to prescribe buprenorphine.
✘✔
This statement is true. Buprenorphine is a schedule III medication. Prescribers must be registered with the DEA to prescribe buprenorphine.
Providers are required to have a DEA X-waiver in order to prescribe buprenorphine.
✘✔
This statement is false. After enactment of the Consolidated Appropriations Act of 2023, Congress eliminated the DATA-Waiver program. Going forward, all prescriptions for buprenorphine only require a standard DEA registration number.
27
The DEA places limits on the number of patients that advanced practice providers are able to see and prescribe buprenorphine.
✘✔
This statement is false. After enactment of the Consolidated Appropriations Act of 2023, there are no longer limitations, under federal law, on the number of patients with OUD that a practitioner may treat with buprenorphine.
27
Buprenorphine has been shown to be diverted more frequently than oxycodone and hydrocodone.
✘✔
This statement is false. Diversion and misuse of buprenorphine products occurs at lower rates than many pharmacists and others assume.
4,5
Buprenorphine has been shown to be diverted less frequently than oxycodone and hydrocodone.
6
SAMHSA. TIP 63: Medications for Opioid Use Disorder. Published online 2021. Accessed August 1, 2021. https://www.cdc.gov/drugoverdose/pdf/pubs/2018-evidence-based-strategies.pdf
Chilcoat HD, Amick HR, Sherwood MR, Dunn KE. Buprenorphine in the United States: Motives for abuse, misuse, and diversion. Journal of Substance Abuse Treatment. 2019;104:148-157. doi:10.1016/j.jsat.2019.07.005
Cicero TJ, Ellis MS, Chilcoat HD. Understanding the use of diverted buprenorphine. Drug and Alcohol Dependence. 2018;193:117-123. doi:10.1016/j.drugalcdep.2018.09.007
Dart RC. Per A New Frontier: Prescription Drug Abuse Beyond Opioids. Presented at: Researched Abuse, Diversion and Addiction-Related Surveillance (RADARS) System 2020 14th Annual Scientific Meeting; n.d.
Reasons for diversion
Inability to obtain prescribed buprenorphine can contribute to diversion.4,5
Chilcoat HD, Amick HR, Sherwood MR, Dunn KE. Buprenorphine in the United States: Motives for abuse, misuse, and diversion. Journal of Substance Abuse Treatment. 2019;104:148-157. doi:10.1016/j.jsat.2019.07.005
Cicero TJ, Ellis MS, Chilcoat HD. Understanding the use of diverted buprenorphine. Drug and Alcohol Dependence. 2018;193:117-123. doi:10.1016/j.drugalcdep.2018.09.007
Studies indicate that patients take buprenorphine without a prescription for therapeutic reasons, such as to reduce withdrawal symptoms, treat pain, manage psychiatric issues, and to wean off opioids.4,7
Chilcoat HD, Amick HR, Sherwood MR, Dunn KE. Buprenorphine in the United States: Motives for abuse, misuse, and diversion. Journal of Substance Abuse Treatment. 2019;104:148-157. doi:10.1016/j.jsat.2019.07.005
Carroll JJ, Rich JD, Green TC. The More Things Change: Buprenorphine/naloxone Diversion Continues While Treatment Remains Inaccessible. J Addict Med. 2018;12(6):459-465. doi:10.1097/ADM.0000000000000436
Among people reporting use of diverted buprenorphine, the most common reasons were to prevent withdrawal (79%), maintain abstinence from opioids (67%), or wean off drugs (3%).
Among respondents who had used diverted buprenorphine, 33% reported barriers to finding a doctor or obtaining buprenorphine on their own.
The majority (81%) indicated they would prefer using prescribed buprenorphine, if available.5
Cicero TJ, Ellis MS, Chilcoat HD. Understanding the use of diverted buprenorphine. Drug and Alcohol Dependence. 2018;193:117-123. doi:10.1016/j.drugalcdep.2018.09.007
Previous use of non-prescribed buprenorphine is associated with greater likelihood of subsequent treatment success.8
Monico LB, Mitchell SG, Gryczynski J, et al. Prior Experience with Non-Prescribed Buprenorphine: Role in Treatment Entry and Retention. Journal of Substance Abuse Treatment. 2015;57:57-62. doi:10.1016/j.jsat.2015.04.010
Combination vs. mono buprenorphine products
As shown in the table below, it may be appropriate for a patient to receive a buprenorphine mono product script for a range of reasons (as opposed to the combination product containing naloxone). The ultimate decision on formulation is the prescriber’s. As of late 2021, the DEA and the Department of Justice demonstrated a preference for pharmacies to document a reason for dispensing mono-product buprenorphine. The prescriber can provide rationale with the script. If not, a pharmacist can inquire and document the response. EXAMPLE RATIONALE: “Patient has experienced an adverse reaction to naloxone”
Combination and Mono Product Buprenorphine: Reasons for Each Script
Combination productBuprenorphine/naloxone
Mono productBuprenorphine
Preferred for both withdrawal management and treatment of OUD9
The ASAM National Practice Guideline for the Treatment of Opioid Use Disorder: 2020 Focused Update. Journal of Addiction Medicine. 2020;14(2S):1-91. doi:10.1097/ADM.0000000000000633
Trainings for SUD treatment providers may recommend prescribing combo product.
Proven safe in pregnancy10,11 and recommended by some perinatal substance use treatment programs12
Linke S, Harrison R, Wallace P. A Web-based intervention used in general practice for people with excessive alcohol consumption. J Telemed Telecare. 2005;11 Suppl 1:39-41. doi:10.1258/1357633054461895
Debelak K, Morrone WR, O’grady KE, Jones HE. Buprenorphine+ naloxone in the treatment of opioid dependence during pregnancy—initial patient care and outcome data. The American journal on addictions. 2013;22(3):252-254.
Project CARA. Use of Buprenorphine -Naloxone in Pregnancy (Project CARA Brief). Published online 2021.
Less likely to be used other than as prescribed
Patient has naloxone allergy or intolerance (nausea, vomiting) or sensitivity to buccal film materials13,14
Strickland DM, Burson JK. Sublingual absorption of naloxone in a large clinical population. J Drug Metab Toxicol. 2018;9(02):240.
Blazes CK, Morrow JD. Reconsidering the usefulness of adding naloxone to buprenorphine. Frontiers in Psychiatry. 2020;11:958.
Reasons that apply to both combo and mono products
May be covered by insurance, or require prior authorization when the other product is not
May cost less via a patient assistance program
Patient was stable on mono product and transferred care to new prescriber; new prescriber decides not to change script
Patients may tolerate one better than the other, or vice versa
For a comprehensive list of buprenorphine product formulations available as of June 2024, please see Resources.